

April 17, 2026
Obstructive sleep apnea (OSA) affects an estimated 30 million Americans.1 OSA is commonly diagnosed and graded using the apnea-hypopnea index (AHI). In practice, however, the AHI reported for the same sleep study may differ depending on which hypopnea criterion is used during scoring. This is why clinicians, laboratories, and payers may refer to AHI-3 and/or AHI-4 when discussing the same patient’s study results. Differences between these two values can affect diagnostic thresholds, severity classification, and insurance reimbursement guidelines.
What is the Apnea-Hypopnea Index?
The Apnea-Hypopnea Index (AHI) is the average number of apneas (complete cessation of airflow) and hypopneas (partial reduction in airflow) per hour of sleep.2 The AHI determines disease severity according to AASM guidelines:
- Normal: AHI < 5 events/hour
- Mild OSA: AHI 5-14 events/hour
- Moderate OSA: AHI 15-29 events/hour
- Severe OSA: AHI ≥ 30 events/hour 2
Importantly, AHI-3 and AHI-4 do not represent two different sleep studies; rather, they are two versions of the apnea-hypopnea index, with the same definition of apnea, differing only in the scoring method for hypopnea.
The Two Hypopnea Scoring Rulesetations
AHI-3
The American Academy of Sleep Medicine (AASM) recommended rule, established in the 2012 scoring manual update, defines a hypopnea as:
A ≥30% reduction in airflow lasting ≥10 seconds, associated with either a ≥3% oxygen desaturation OR an arousal from sleep.2
AHI-4
The AHI-4, AASM acceptable rule, historically aligned with Centers for Medicare & Medicaid Services (CMS) requirements, defines a hypopnea as:
A ≥30% reduction in airflow lasting ≥10 seconds, associated with a ≥4% oxygen desaturation.2
This more stringent criterion focuses on events with clear physiological consequences, specifically significant drops in blood oxygen levels. The rationale behind this threshold centers on capturing events with demonstrable cardiovascular and metabolic implications.3
Clinical Implications of the Two Scoring Methods
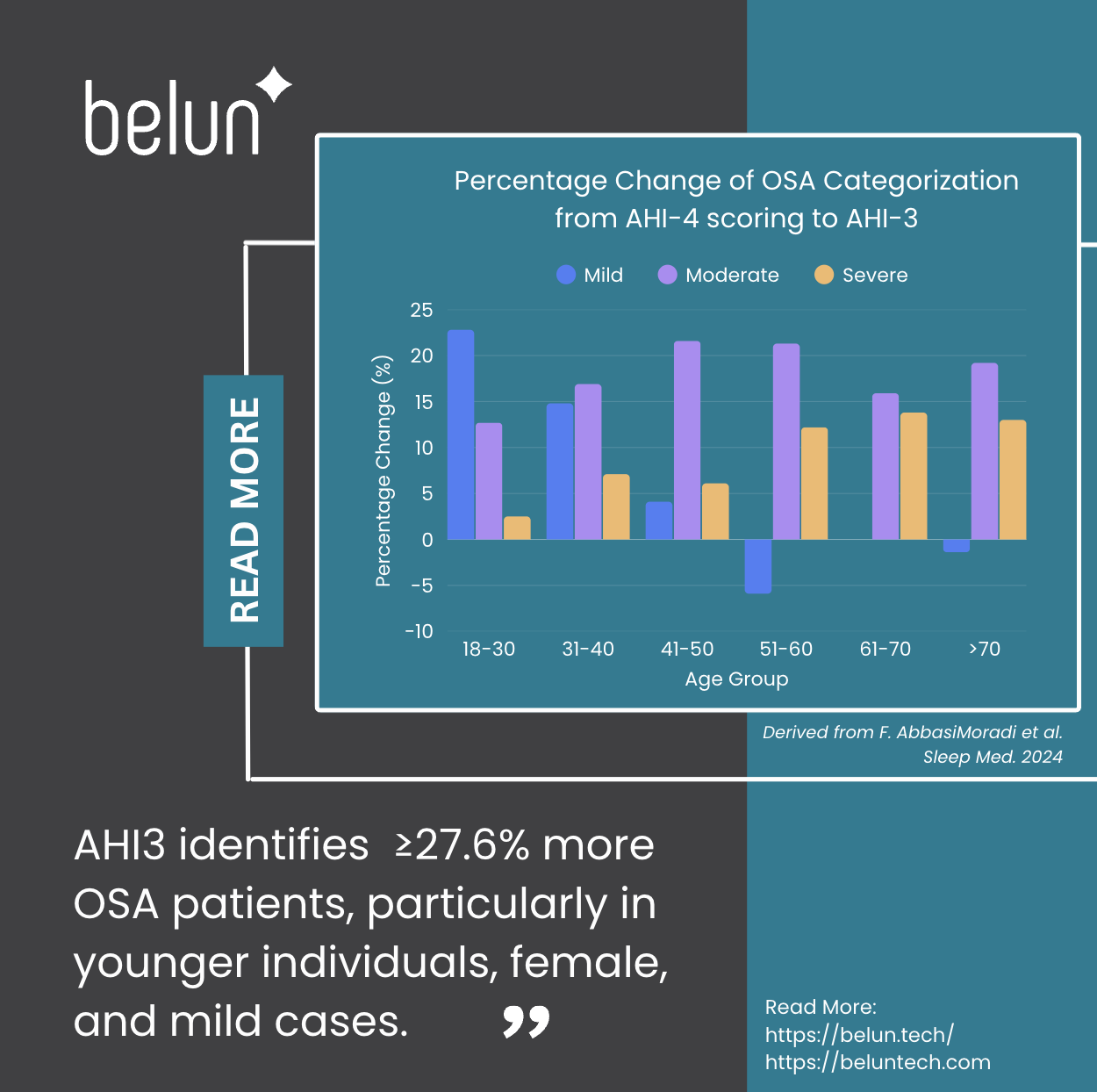
The choice between AHI-3 and AHI-4 scoring can dramatically affect diagnostic outcomes, particularly across different age groups. According to Abbasi-Moradi et al. in Sleep Medicine (2024) ,4 changing from the 4% criterion to the updated 3% recommended rule increases OSA diagnosis rates by approximately 27.6% to 38.8% across different age groups(Table 1). 4 This surge in positive diagnoses is particularly prominent among patients under age 40 with mild OSA symptoms — a finding that underscores the importance of screening younger patients who may exhibit relatively healthier oxygen desaturation patterns than older OSA patients yet demonstrate alarming arousal patterns (Figure. 1).
Table 1: According to F. AbbasiMoradi et al. 2024, Age-stratified percentage change in OSA severity classification after switching from AHI-4 to AHI-3
Delta Difference% in diagnosis from 4%AHI to 3%AHI
| Age | 18-30 N=79 | 31-40 N=183 | 41-50 N=245 | 51-60 N=272 | 61-70 N=276 | >70 N=146 |
| Normal | -38.0% | -38.8% | -31.8% | -27.6% | -29.7% | -30.8% |
| Mild | +22.8% | +14.8% | +4.1% | -5.9% | +0.0% | -1.4% |
| Moderate | +12.7% | +16.9% | +21.6% | +21.3% | +15.9% | +19.2% |
| Severe | +2.5% | +7.1% | +6.1% | +12.2% | +13.8% | +13.0% |
Figure 1: According to F. AbbasiMoradi et al. 2024, graphical representation of the increase in diagnosis of subjects under the updated AASM recommendation rule (AHI-3) from AHI-4 criteria:

Derived from table 2, Abbasi-Moradi et al. 2024
Diagnostic Sensitivity
The AHI-3 rule demonstrates higher sensitivity in detecting:
- Sleep apnea in younger patients with shallower oxygen desaturation pattern4
- Case report where upper airway resistance causes arousals without significant desaturation5
- REM-related sleep apnea, where events may cause arousals without deep desaturations (especially in women and young patients)6–10
Population-Specific Considerations
As mentioned before, the following populations show particular vulnerability to underdiagnosis when using AHI-4:
- Women: Often present with more arousals, less severe OSA during NREM, and greater respiratory events during REM.10,11
- Younger adults: May have greater respiratory reserve, limiting desaturation.12
- Patients with comorbid COPD: Complex interactions between respiratory conditions,13 often resulting in more arousals and difficulty falling asleep.
Practical Challenges and Controversies
Sleep laboratories face practical challenges in navigating these dual standards. Recommended approaches include:
- Dual reporting: Providing both AHI-3 and AHI-4 values on every case
- AASM-standard reporting: Using recommended criteria with supplementary data for insurance policy
Future Technological Directions
Emerging technologies may influence future diagnostic paradigms:
- Hypoxic burden calculations: Quantifying total oxygen deficit rather than event counting14 (Stay tuned for future blog posts where we will dive into why measuring the hypoxic burden is so critical.)
- Multi-night testing: Capturing night-to-night variability in AHI
What Belun Offers?
Belun Ring provides multi-night Level 3 Sleep test, providing both AHI-3 and AHI-4 scoring and also hypoxic burden, providing more comprehensive phenotyping of patients’ sleep disorders and enabling long-term monitoring of treatment effects.
Key Takeaways: Guidelines for Applying AHI-3 vs. AHI-4 Criteria
AHI-3 is recommended for:
- Initial clinical diagnosis: Particularly for highly symptomatic patients presenting with a sub-threshold AHI.
- Atypical presentations: Specifically, younger patients with a low-to-moderate BMI who exhibit marked daytime fatigue despite minimal oxygen desaturation.
- Targeted demographics: Women with suspected REM-predominant OSA.
AHI-4 is recommended for:
- Cardiovascular risk assessment: When the clinical focus requires identifying events with a more evident hypoxic burden.
- Administrative compliance: Fulfilling documentation requirements for Medicare, payer preauthorization, or PAP therapy reimbursement.
- Longitudinal analysis: Facilitating historical comparisons with older sleep studies, prior clinical reports, or legacy databases.
Conclusion
The distinction between AHI-3 and AHI-4 scoring rules represents more than a technical detail—it fundamentally affects which demographic differences in patients receive diagnoses and access to treatment. AHI3 offers greater sensitivity and better reflects the full spectrum of obstructive sleep apnea pathophysiology, AHI4 creates coverage challenges for these subsets of patients, in particular to younger and female patients with less steep oxygen desaturation patterns and more arousals. Until standardization occurs, the sleep medicine community must remain vigilant in ensuring that scoring methodology differences do not create barriers to necessary care for patients with obstructive sleep apnea.
REFERENCE:
1. Benjafield, A. V. et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir. Med. 7, 687–698 (2019).
2. Berry, R. B. et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events: deliberations of the Sleep Apnea definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 08, 597–619 (2012).
3. Punjabi, N. M., Newman, A. B., Young, T. B., Resnick, H. E. & Sanders, M. H. Sleep-disordered breathing and cardiovascular disease: an outcome-based definition of hypopneas. Am. J. Respir. Crit. Care Med. 177, 1150–1155 (2008).
4. AbbasiMoradi, F., Mogavero, M. P., Palomino, M., Ferri, R. & DelRosso, L. M. Age related disparities in sleep apnea diagnosis using a wearable device: Implications of 4% vs. 3% hypopnea scoring criteria. Sleep Med. 118, 88–92 (2024).
5. Guilleminault, C., Stoohs, R., Clerk, A., Cetel, M. & Maistros, P. A cause of excessive daytime sleepiness. The upper airway resistance syndrome. Chest 104, 781–787 (1993).
6. Mokhlesi, B. & Punjabi, N. M. “REM-related” Obstructive Sleep Apnea: An Epiphenomenon or a Clinically Important Entity? Sleep 35, 5–7 (2012).
7. Resta, O. et al. Gender difference in sleep profile of severely obese patients with obstructive sleep apnea (OSA). Respir. Med. 99, 91–96 (2005).
8. Koo, B. B., Patel, S. R., Strohl, K. & Hoffstein, V. Rapid eye movement-related sleep-disordered breathing: influence of age and gender. Chest 134, 1156–1161 (2008).
9. Goh, D. Y., Galster, P. & Marcus, C. L. Sleep architecture and respiratory disturbances in children with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 162, 682–686 (2000).
10. O’Connor, C., Thornley, K. S. & Hanly, P. J. Gender Differences in the Polysomnographic Features of Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 161, 1465–1472 (2000).
11. Ye, L., Pien, G. W. & Weaver, T. E. Gender differences in the clinical manifestation of obstructive sleep apnea. Sleep Med. 10, 1075–1084 (2009).
12. Heinzer, R. et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir. Med. 3, 310–318 (2015).
13. Owens, R. L. & Malhotra, A. Sleep-disordered breathing and COPD: the overlap syndrome. Respir. Care 55, 1333–1344; discussion 1344-1346 (2010).
14. Azarbarzin, A. et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study. Eur. Heart J. 40, 1149–1157 (2019).
Publications by Belun :
1) “Belun® Ring Platform: a novel home sleep apnea testing system for assessment of obstructive sleep apnea” (https://jcsm.aasm.org/doi/10.5664/jcsm.8592),
2) “Detection of obstructive sleep apnea using Belun® Sleep Platform wearable with neural network based algorithm and its combined use with STOP-Bang questionnaire” (https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0258040),
3) “Belun® Ring (Belun® Sleep System BLS-100): Deep Learning-Facilitated Wearable Enables OSA Detection, Apnea Severity Categorization, and Sleep Stage Classification in Patients Suspected of OSA” (https://pubmed.ncbi.nlm.nih.gov/37380590/),
4) “Correlation of Pulse Rate Variability(PRV) and Heart Rate Variability(HRV) Metrics During Sleep in Subjects Suspected of OSA” (https://academic.oup.com/sleep/article/46/Supplement_1/A420/7182347)
5) “The Belun sleep platform to diagnose obstructive sleep apnea in patients with hypertension and high cardiovascular risk” (https://pubmed.ncbi.nlm.nih.gov/37071415/)
6) “Integrating Body Sensor into a Wearable Platform to Enhance the Identification of Central and Mixed Apneas”. (https://academic.oup.com/sleep/article/47/Supplement_1/A222/7654683)
7) “Using a Wearable’s Multi-Night Capability to Mitigate Night-to-Night Variability in a Dental Clinic Cohort”. J Dental Sleep Med. 2026; 13(1). (https://aadsm.org/journal/original_article_1_issue_131.php)
Partnering with Belun :
If you would like to know more about how to adopt Belun’s solution in your organization, please feel free to contact us to schedule a meeting by filling out the form below:

